When you’re struggling with severe obesity, losing weight isn’t just about willpower. It’s about biology. Your body fights back-hormones signal hunger, metabolism slows, and even the most disciplined diets often fail. That’s where bariatric surgery comes in. Two procedures dominate the field: gastric bypass and sleeve gastrectomy. Both work. Both change your life. But they’re not the same. And choosing between them isn’t just about which one loses more weight-it’s about which one fits your body, your health, and your long-term future.
How They Work: Restrict vs. Restrict and Redirect
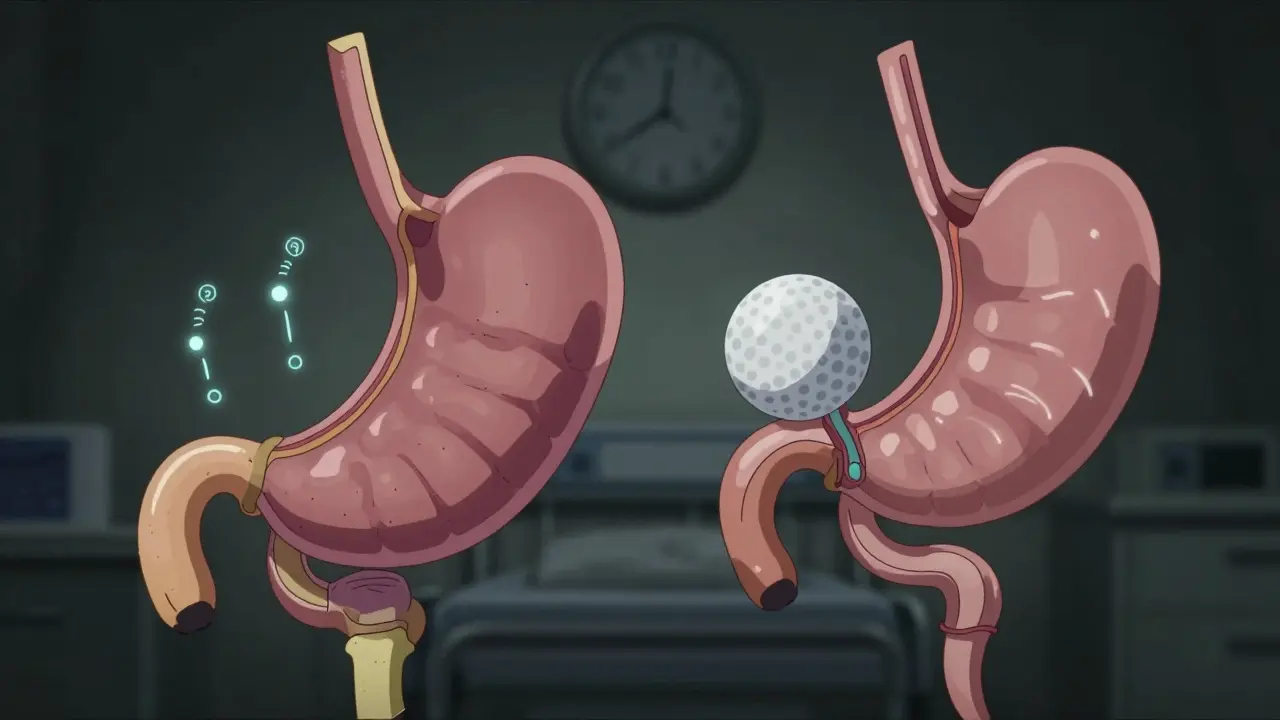
Gastric bypass and sleeve gastrectomy both shrink your stomach, but they do it in completely different ways. With sleeve gastrectomy, surgeons remove about 80% of your stomach, leaving behind a narrow tube shaped like a banana. That’s it. No rerouting. Just a smaller stomach that fills up faster and sends fewer hunger signals. The procedure takes about 47 minutes on average and is done entirely laparoscopically. Recovery is quick-most people leave the hospital the next day.
Gastric bypass is more complex. Surgeons create a small pouch, about the size of a golf ball, from the top of your stomach. Then they cut the small intestine and reconnect it to this new pouch, bypassing most of the stomach and the first part of the intestine. This isn’t just about size-it’s about changing how food moves through your body. Food skips the parts that normally absorb calories and nutrients. That’s why gastric bypass is called a malabsorptive procedure. It takes longer-about 68 minutes on average-and requires more precision.
Weight Loss: Faster and Deeper With Bypass
If your goal is to lose the most weight as quickly as possible, gastric bypass usually wins. Studies show patients lose 57% of their excess weight at the five-year mark with bypass, compared to 49% with sleeve. Some patients see 60-80% of excess weight gone within the first 18 months with bypass. Sleeve patients lose 60-70% over the same period, but it tends to happen more slowly.
Why the difference? It’s not just the smaller stomach. The bypass changes how your gut hormones work. It reduces ghrelin-the hunger hormone-more than sleeve does. It also alters signals that tell your brain you’re full. This isn’t just about feeling full faster. It’s about your brain no longer craving sugar or carbs the way it used to. That’s why many patients say they suddenly lose interest in junk food after bypass.
Long-Term Risks: Safety vs. Revisions
Here’s where things get complicated. Sleeve gastrectomy is safer in the short term. A 2022 study of over 95,000 Medicare patients found that five years after surgery, the risk of death was 32.8% lower for sleeve patients than for bypass patients. Complications like infections, bleeding, and leaks are also less common with sleeve.
But here’s the twist: sleeve patients are more likely to need a second surgery. About 3.2 percentage points more sleeve patients end up needing a revision within five years. Why? Weight regain. Some people’s stomachs stretch over time. Others don’t lose enough weight and end up back in the doctor’s office asking, “Can I get bypass now?”
Gastric bypass, on the other hand, holds its results better long-term. Fewer people regain weight. But it comes with its own risks. Internal hernias used to be common, but modern techniques now close off the spaces where they can form-cutting hernia rates from 5% to under 1%. Still, bypass patients face lifelong risks of nutrient deficiencies.
Nutrition: Lifelong Supplements Are Non-Negotiable
If you choose gastric bypass, you will need to take vitamins for the rest of your life. Bypass reduces your body’s ability to absorb iron, calcium, vitamin B12, and folate. Without supplements, you risk anemia, nerve damage, and bone loss. Blood tests every six months aren’t optional-they’re mandatory. Some patients still develop deficiencies even with strict adherence.
Sleeve gastrectomy doesn’t cause malabsorption. That’s why it’s become the most popular procedure in the U.S., accounting for over 60% of all bariatric surgeries in 2023. You still need to take vitamins-especially B12 and iron-but the doses are lower, and the monitoring is less intense. Annual blood tests are often enough.
One major downside of sleeve? It can worsen acid reflux. About 15-20% of sleeve patients develop new or worse GERD after surgery. Gastric bypass, surprisingly, often improves reflux. That’s why doctors sometimes recommend bypass for patients with severe heartburn.
Quality of Life: Hunger, Dumping, and Daily Habits
On Reddit’s r/bariatrics, a thread with over 1,200 comments from early 2024 revealed a clear pattern. Sleeve patients often say: “I recovered faster. I didn’t feel sick after eating.” But many also say: “I still feel hungry. I snack. I gain back a few pounds.”
Gastric bypass patients, meanwhile, talk about “dumping syndrome”-a sudden wave of nausea, sweating, dizziness, and diarrhea that hits after eating sugary or fatty foods. Up to 70% of bypass patients experience it. At first, it’s terrifying. But over time, most learn to avoid trigger foods. And many say it’s the best thing that ever happened to them. “I used to eat ice cream every night,” one patient wrote. “Now I can’t even look at it. I don’t even want it.”
RealSelf.com reviews show 91% of bypass patients say the surgery was “worth it,” compared to 89% for sleeve. But the bypass group also reports more complications. It’s a trade-off: better results, more risks.
Cost and Insurance: What You’ll Pay
Out-of-pocket costs for sleeve gastrectomy average $14,500. For gastric bypass, it’s $19,300. That’s a $4,800 difference. Insurance usually covers 80% of both procedures if you meet the criteria: BMI ≥40, or BMI ≥35 with conditions like diabetes, high blood pressure, or sleep apnea. Some insurers, like UnitedHealthcare, now require BMI ≥45 as of early 2024.
Pre-op requirements are identical: six months of documented weight loss attempts, psychological screening, and medical clearance. Post-op, both require a strict diet progression-from liquids to purees to solid foods over several weeks. But bypass patients have more restrictions: no sugar, no alcohol, no carbonated drinks. Sleeve patients can often drink soda and eat sweets, at least early on. That’s why some people choose sleeve thinking it’s “easier.” But they don’t always realize how much they’ll still need to change.
Who Gets Which Surgery?
There’s no one-size-fits-all. But here’s how most surgeons decide:
- Choose gastric bypass if you have type 2 diabetes, severe GERD, or need the most dramatic weight loss. It’s also better if you’re at high risk for long-term weight regain.
- Choose sleeve gastrectomy if you want a simpler procedure, fewer nutrient issues, and faster recovery. It’s ideal if you’re healthy otherwise and want to avoid lifelong supplement dependency.
One growing trend: surgeons are starting to combine the two. A new procedure called the “sleeve with bypass” or “mini-bypass” is being tested at major centers like Mayo Clinic and Massachusetts General. It uses the sleeve’s simplicity but adds a short bypass to boost weight loss and diabetes control. Early results look promising.
The Bottom Line
Neither surgery is magic. Both require lifelong changes. But if you’re serious about reversing the damage of severe obesity, one of them can give you back your health. Gastric bypass gives you more weight loss and better metabolic results-but at a higher cost, more risk, and more responsibility. Sleeve gastrectomy is safer, simpler, and easier to live with-but you might need a second surgery down the road.
There’s no perfect choice. Only the right one for you.
Which surgery leads to more weight loss: gastric bypass or sleeve gastrectomy?
Gastric bypass typically leads to more weight loss. Studies show patients lose about 57% of their excess weight at the five-year mark with bypass, compared to 49% with sleeve gastrectomy. Some patients lose 60-80% of excess weight within 18 months with bypass, while sleeve patients usually lose 60-70% over the same period, but at a slower pace.
Is sleeve gastrectomy safer than gastric bypass?
Yes, sleeve gastrectomy is generally safer in the short term. A 2022 study of over 95,000 patients found a 32.8% lower risk of death at five years for sleeve patients compared to bypass patients. Complications like infections and leaks are also less common with sleeve. However, sleeve patients are more likely to need revision surgery later due to weight regain or stomach stretching.
Do I have to take vitamins for life after bariatric surgery?
After gastric bypass, yes-you’ll need lifelong supplements for iron, calcium, vitamin B12, and folate due to malabsorption. Blood tests every six months are required. After sleeve gastrectomy, you still need vitamins, but the risk of deficiency is lower. Annual blood tests are often sufficient, and you won’t need as many supplements.
Can bariatric surgery cure type 2 diabetes?
Yes, both surgeries can lead to diabetes remission, but gastric bypass is more effective. The malabsorptive component of bypass improves insulin sensitivity and reduces blood sugar more dramatically than sleeve. Studies show up to 80% of bypass patients achieve normal blood sugar without medication, compared to 60-70% with sleeve.
Why is sleeve gastrectomy more popular than gastric bypass?
Sleeve gastrectomy is simpler, faster, and has fewer long-term nutritional risks. It doesn’t reroute the intestines, so there’s no malabsorption. Recovery is quicker, and patients report fewer side effects like dumping syndrome. In 2023, sleeve made up 63.2% of all bariatric surgeries in the U.S., up from under 10% in 2010, while bypass dropped from 31% to 27.4%.
What’s the risk of needing a second surgery after bariatric surgery?
Sleeve gastrectomy patients are more likely to need revision surgery-about 3.2 percentage points higher than bypass patients within five years. This is often due to weight regain, stomach stretching, or worsening GERD. Gastric bypass has a lower revision rate because it holds weight loss better, though it carries higher risks of complications like internal hernias or nutrient deficiencies.
Aisling Maguire
February 28, 2026 AT 22:29So I had the sleeve last year and honestly? It was a game-changer. No dumping, no crazy side effects. I still get hungry sometimes, but it’s manageable. The recovery was a breeze - back to work in a week. I do take B12 and iron, but honestly? It’s way easier than I thought. I’m down 70 lbs and finally feel like myself again.
Justin Ransburg
March 1, 2026 AT 19:44Thank you for this comprehensive breakdown. The data presented here is both clinically sound and accessible to the layperson. It is imperative that patients understand that bariatric surgery is not a panacea, but rather a tool that demands lifelong commitment to nutritional integrity and behavioral adaptation. The comparative outcomes between sleeve and bypass underscore the necessity of individualized care pathways grounded in evidence-based medicine.
Sumit Mohan Saxena
March 3, 2026 AT 05:53As a gastroenterologist with over 15 years in bariatric care, I can confirm the data presented. Sleeve gastrectomy has indeed become the most prevalent procedure due to its favorable safety profile and technical reproducibility. However, the long-term metabolic advantages of gastric bypass - particularly in patients with type 2 diabetes and severe GERD - remain unmatched. The emerging ‘mini-bypass’ hybrid technique shows promise in bridging the gap between efficacy and safety. Multicenter trials are ongoing at Mayo and Mass General, with preliminary results suggesting a 6% higher remission rate for diabetes at three years compared to sleeve alone.
Ben Estella
March 4, 2026 AT 19:45Let’s be real - if you’re gonna do this, go full bypass. Sleeve is for people who want to take the easy way out. You think you’re avoiding supplements? You’re just setting yourself up for a second surgery in five years. Bypass doesn’t play around. You eat sugar? You puke. You eat greasy food? You collapse. It’s not a punishment - it’s biology reprogramming your brain. And yeah, you’ll need vitamins. So what? You’re not a toddler. Take your damn pills. This isn’t a spa retreat - it’s a life-saving intervention.
Sneha Mahapatra
March 5, 2026 AT 06:09I read this with tears in my eyes. My sister had sleeve last year. She went from being too tired to play with her kids to hiking 10 miles on weekends. But I also see how hard it is - the hunger, the cravings, the fear of slipping back. I think what’s missing from this conversation is the emotional toll. It’s not just about weight. It’s about grief - for the old body, the old habits, the old self. I wish more people talked about that. Not just the numbers. The quiet moments. The loneliness. The pride.
bill cook
March 6, 2026 AT 10:22Wait so if I do sleeve and then gain weight back, can I just get bypass later? Like, is that even allowed? My cousin did sleeve and now she’s back to 300 lbs and crying every night. She says she regrets it. Shouldn’t they warn people better? Like, maybe they should show you a video of someone who did sleeve and then had to redo it. That’d scare people straight.
Katherine Farmer
March 7, 2026 AT 03:06How quaint. The American healthcare system reduces life-altering metabolic interventions to a simplistic cost-benefit spreadsheet. ‘Which one loses more weight?’ as if this were a grocery store aisle. The real issue isn’t the procedure - it’s the cultural delusion that surgery can fix a problem rooted in systemic neglect, food deserts, and psychiatric comorbidities. You think a stomach reduction will cure trauma? Please. The fact that we treat obesity as a mechanical flaw rather than a sociological catastrophe is the true tragedy.
Full Scale Webmaster
March 7, 2026 AT 05:40Okay so I’ve been on both sides of this and I need to say something. I had bypass in 2019. Lost 120 lbs. Then in 2022 I had a hernia. Then in 2023 I got a bowel obstruction. Then in 2024 I found out I’m deficient in vitamin D, B12, iron, zinc, and magnesium. My doctor says I need to take 17 pills a day. I can’t drink soda. I can’t have dessert. I can’t even have coffee with cream. I used to love tacos. Now I cry when I smell them. And guess what? My sister did sleeve. She eats pizza every Friday. She’s down 50 lbs. She’s happy. She’s not in the hospital. She’s not on a pill regimen. She’s not depressed. And she’s not a failure. So stop acting like bypass is the gold standard. It’s not. It’s a gamble. And some of us lost.
Lisa Fremder
March 9, 2026 AT 03:15Why do we even have two options? Just make everyone do bypass. It works better. End of story. People who choose sleeve are just weak. They want the quick fix. They don’t want to deal with the real change. I’m 300 lbs and I’m not even going to bother. I know I’d be the one crying in the hospital after the hernia. So I’m just gonna keep eating. Why fight it?
Byron Duvall
March 10, 2026 AT 11:41Did you know the FDA approved these surgeries because Big Pharma wanted more vitamin sales? They made a deal with the surgeons. The supplements? That’s where the real profit is. You think they care about your health? They care about your B12 prescriptions. And the insurance companies? They only cover it because it’s cheaper than treating diabetes for life. This whole thing is a racket. They don’t want you healthy. They want you dependent.
Brandie Bradshaw
March 12, 2026 AT 02:29It’s important to recognize that the rhetoric surrounding bariatric surgery often oversimplifies a profoundly complex physiological, psychological, and socioeconomic phenomenon. The notion that one procedure is ‘better’ than another ignores the heterogeneity of patient biology, psychosocial context, and postoperative support structures. Furthermore, the emphasis on weight loss percentages as a primary outcome metric is not only reductive - it is ethically suspect. What of quality of life? Mental health outcomes? Long-term functional capacity? These metrics are rarely measured with the same rigor - and yet, they are the true indicators of success.
Sophia Rafiq
March 12, 2026 AT 14:57Got sleeve. 8 months in. Lost 65 lbs. No dumping. No crazy rules. I still eat carbs. I still have wine. I snack sometimes. But I don’t binge. My energy is insane. My knees don’t hurt. I started running. I didn’t even know I could. I’m not ‘cured.’ But I’m alive again. And honestly? That’s enough.
Martin Halpin
March 13, 2026 AT 23:01You all are missing the point. The real issue isn’t bypass vs. sleeve - it’s that we treat obesity like a personal failure. You think people choose to be obese? They didn’t wake up one day and say, ‘Hey, I’m gonna eat 5000 calories a day and sit on the couch.’ They were raised on processed food. They work two jobs. They don’t have time to cook. They’re stressed. They’re lonely. They’re traumatized. Surgery doesn’t fix that. It just moves the problem from the stomach to the soul. And then we pat ourselves on the back for ‘fixing’ them. We’re not healers. We’re just good at putting Band-Aids on bullet wounds.