
Imagine rolling over in bed to check the time, only to feel like the room is spinning violently around you. You freeze, heart racing, waiting for the world to stop tilting. This isn't a stroke or a heart attack-it’s likely BPPV, also known as Benign Paroxysmal Positional Vertigo. It is a common inner ear disorder caused by displaced calcium crystals that send false motion signals to your brain. While the name sounds complex, the condition is actually quite straightforward to understand and, most importantly, highly treatable.
BPPV is the leading cause of peripheral vertigo, accounting for more than half of all cases seen in clinics. Despite being labeled "benign" because it is not life-threatening, the impact on daily life can be severe. Episodes are brief-usually lasting less than a minute-but they are intense enough to cause nausea, falls, and significant anxiety. The good news? You don’t need surgery or long-term medication to fix it. A simple physical maneuver called Canalith Repositioning is a series of head movements designed to guide loose inner ear crystals back to their proper place often resolves the issue in one session.
The Inner Ear: Where the Problem Starts
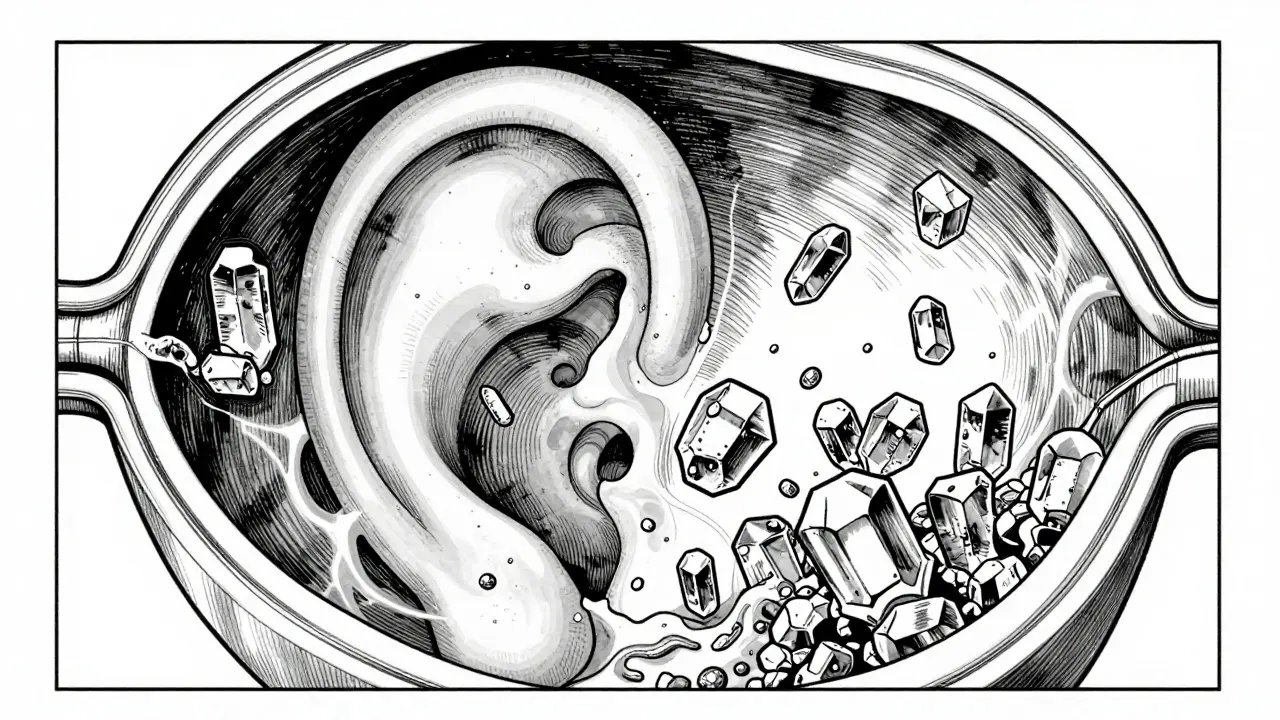
To understand why you feel dizzy, we need to look inside your ear. Your balance system relies on two main parts: the vestibular system (for balance) and the cochlea (for hearing). Inside the vestibular system, you have three semicircular canals filled with fluid. These canals detect rotational head movements. When you turn your head, the fluid moves, bending tiny hair cells that signal your brain about your position in space.
Normally, small calcium carbonate crystals called otoconia are microscopic particles located in the utricle of the inner ear that help detect linear acceleration and gravity sit in a gel-like sac called the utricle. They act like sand in an hourglass, helping you sense tilt and gravity. In BPPV, these crystals break loose. Think of them as sediment that has washed out of its designated pool and drifted into one of the semicircular canals.
When these free-floating crystals end up in a canal, they disrupt the fluid flow. Gravity pulls the heavy crystals down, dragging the fluid with them even when your head is still. This sends a false signal to your brain that you are spinning, even though you are sitting perfectly still. This mismatch between what your eyes see and what your inner ear feels creates the sensation of vertigo.
Who Gets BPPV and Why?
You might wonder if you did something wrong to trigger this. In many cases, there is no single clear cause. However, several factors increase your risk:
- Aging: BPPV is most common in adults between 50 and 70 years old. As we age, the structures in our inner ear become more fragile, making crystal dislodgement more likely.
- Gender: Women are 1.5 to 2 times more likely to develop BPPV than men. Researchers believe hormonal changes or bone density issues may play a role.
- Head Trauma: Even mild bumps to the head can shake loose otoconia. If you’ve had a concussion or whiplash, watch for delayed dizziness.
- Vitamin D Deficiency: Recent studies suggest a link between low vitamin D levels and recurrent BPPV. Vitamin D helps maintain healthy calcium metabolism in the inner ear.
- Sedentary Lifestyle: Lack of movement may allow crystals to settle and clump, increasing the chance of displacement.
It’s worth noting that BPPV is rarely linked to serious neurological conditions. Unlike central vertigo (caused by brain issues), BPPV is strictly mechanical. It’s a plumbing problem in your ear, not a wiring problem in your brain.
Spotting the Signs: Is It BPPV?
Not every dizzy spell is BPPV. To identify it correctly, look for these specific characteristics:
- Triggered by Head Position: Symptoms start when you change your head position relative to gravity. Common triggers include rolling over in bed, looking up to reach a shelf, bending down to tie shoes, or quickly turning your head.
- Short Duration: The spinning sensation lasts from 5 seconds to 1 minute. If it goes on for hours or days, it’s probably not BPPV.
- Latency: There’s usually a short delay (2-10 seconds) between moving your head and feeling the vertigo. This happens because the crystals need time to shift within the fluid.
- Fatigability: If you repeat the triggering movement, the dizziness gets weaker or stops entirely. This is because the crystals settle into a new position.
- No Other Neurological Symptoms: BPPV does not cause slurred speech, double vision, weakness in limbs, or loss of consciousness. If you experience these, seek emergency care immediately.
A healthcare provider will confirm the diagnosis using the Dix-Hallpike maneuver is a diagnostic test where the patient is moved from sitting to lying with the head turned and tilted back to provoke vertigo and observe eye movements. During this test, they watch for nystagmus-involuntary eye movements-that confirms which ear and which canal is affected.
How Canalith Repositioning Works
The gold standard treatment for BPPV is not medication, but physical therapy. Specifically, canalith repositioning procedures (CRPs) use gravity to move the loose crystals out of the semicircular canal and back into the utricle, where they belong.
The most famous technique is the Epley maneuver is a sequence of four head positions held for 30-60 seconds each to relocate crystals from the posterior semicircular canal. It works best for posterior canal BPPV, which accounts for 80-90% of cases. Here’s how it typically unfolds:
- Step 1: Sit on the edge of a bed with pillows behind your head. Turn your head 45 degrees toward the affected side.
- Step 2: Lie back quickly so your head rests slightly below the edge of the bed, still turned 45 degrees. Hold this position for 30-60 seconds until the vertigo stops.
- Step 3: Without lifting your head, turn it 90 degrees to the other side. Hold for another 30-60 seconds.
- Step 4: Roll your body onto your side so you are facing the floor. Your nose should point toward the floor. Hold for 30-60 seconds.
- Step 5: Sit up slowly, keeping your chin tucked.
For horizontal canal BPPV (5-10% of cases), providers use the Lempert roll is a repositioning maneuver involving rolling the patient 360 degrees along the longitudinal axis of the body to treat horizontal canal BPPV. For anterior canal BPPV (rare), the Semont maneuver is a rapid lateral decubitus procedure used to treat anterior or posterior canal BPPV by leveraging gravity to dislodge crystals may be recommended.
Success rates are impressive. About 80-90% of patients see improvement after just one session. Some may need a second or third visit if the crystals haven’t fully cleared. Home-based video-guided Epley maneuvers have shown 72% success, making self-treatment a viable option for those who cannot access a specialist quickly.
What Not to Do: Common Mistakes
Many people try to manage BPPV with the wrong tools, which can prolong symptoms or mask underlying issues.
- Don’t Rely on Vestibular Suppressants: Drugs like meclizine or dimenhydrinate reduce dizziness temporarily but do not fix the root cause. In fact, they can slow down your brain’s ability to adapt to the imbalance, potentially worsening recovery.
- Avoid Unnecessary Imaging: MRI scans are expensive and rarely helpful for typical BPPV. They won’t show loose crystals. Save imaging for cases where neurological red flags are present.
- Don’t Ignore Recurrence: BPPV tends to come back. Up to 50% of patients experience recurrence within five years. If it returns, don’t panic-repeat the repositioning maneuver or consult a vestibular therapist.
- Stay Active: Bed rest doesn’t help. Gentle movement encourages your vestibular system to recalibrate. Avoid sudden head jerks, but don’t stay sedentary.

Living with BPPV: Practical Tips
While waiting for treatment or during recovery, small adjustments can make life easier:
- Sleep Propped Up: Use two pillows to keep your head elevated. This reduces the gravitational pull on loose crystals while you sleep.
- Movements Slowly: Change positions gradually. Sit up before standing. Turn your whole body instead of just your head.
- Focus on a Fixed Point: During an episode, stare at a stationary object. This helps your brain reconcile conflicting signals from your eyes and inner ear.
- Prevent Falls: Remove tripping hazards from your home. Use nightlights. Consider a cane if unsteadiness persists.
- Check Vitamin D Levels: Ask your doctor for a blood test. Supplementing with 1,000 IU daily may reduce recurrence risk if you’re deficient.
When to See a Specialist
If you suspect BPPV, start with your primary care provider. However, consider seeing a vestibular specialist if:
- Your symptoms last longer than a minute.
- You have hearing loss, ringing in the ears (tinnitus), or pressure in the ear-these could indicate Meniere’s disease.
- The Epley maneuver doesn’t work after two attempts.
- You have frequent recurrences despite proper treatment.
- You experience headaches, neck pain, or neurological symptoms alongside dizziness.
Vestibular rehabilitation therapists can perform precise diagnostics and tailor exercises to your specific case. Telehealth options have expanded significantly, with virtual guidance showing 68% effectiveness compared to in-person care.
Is BPPV dangerous?
No, BPPV is not life-threatening. It is called "benign" because it does not cause permanent damage to your brain or inner ear. However, it can lead to falls, especially in older adults, so prompt treatment is important for safety.
How long does BPPV last without treatment?
Episodes themselves last seconds to a minute. However, the condition can persist for weeks or months if untreated. Spontaneous resolution occurs in about 40-50% of cases within a month, but treatment speeds up recovery significantly.
Can I do the Epley maneuver at home?
Yes, if you know which ear is affected and have been diagnosed by a professional. Video-guided instructions improve success rates to 72%. If unsure, consult a clinician first to avoid treating the wrong side or aggravating other conditions.
Why does BPPV come back?
Recurrence is common due to aging, minor head trauma, or vitamin D deficiency. Up to 50% of patients experience another episode within five years. Maintaining adequate vitamin D levels and staying physically active may help reduce frequency.
Does BPPV affect hearing?
No, BPPV does not cause hearing loss. If you experience hearing changes, tinnitus, or ear fullness, you may have a different condition like Meniere’s disease or vestibular neuritis, requiring different management.